And so it begins...
I love science fiction. As both a Star Wars fan and a scientist, I often find myself daydreaming of what the future holds for both technology and mankind. As we continue to progress as humans, we will inevitably hit numerous ethical speed bumps (or speed mountains) along the way to becoming the most advanced species in the universe. Want to get to Mars? Live forever? Cure all human disease? All of these things sound great, but these advancements are always tied to some pretty hard choices.

Figure 1: Sometimes the choice won't be this easy! The answer is cake, by the way.
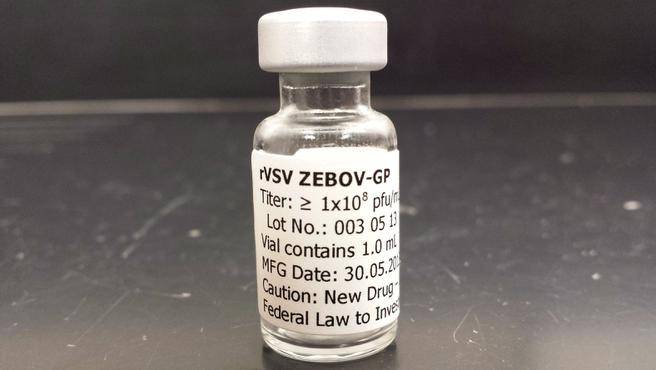
A few months ago, I blogged about how genetic engineering has the potential to help cure a variety of human diseases. I also mentioned how thought leaders in the genetic engineering space proposed that a moratorium be held on any attempts to use such technology to edit a human embryo. Well it seems like that those requests were ignored, as a study was recently published in Protein and Cell attempting to correct the gene that causes beta thalassemia in embryos. This disease results in misshapen hemoglobin, the component of your blood that carries oxygen. Misshapen hemoglobin leads to anemia, so you can see why someone would want to cure it! In the above paper, 86 embryos were used in an attempt to correct the mutation. They used CRISPR/Cas9, a very clever system discovered in 2012 that has the ability to hone in on specific regions of DNA, cut out the gene in question, and replace it with a different one. Only a small number correctly replaced the mutated gene with a normal copy, and the process also generated mutations in other unintended parts of the genome.
Let me be very clear here. The researchers (at least, to my knowledge) never intended to implant these embryos into an actual womb. As controversial as this study was, it actually provides us with important confirmation of what we already suspected - we simply need to learn more about how gene editing technologies like CRISPR/Cas9 work before we can hope to use them in an actual embryo. The success rate for this paper was pretty small. The success rate if we want to start using this routinely? 100%.
This technology has the potential to rid the human race of a whole host of genetic disorders, but the fact that we are still extraordinarily naive about how exactly such technologies will behave in an actual embryo cannot be understated. The majority of scientific institutions throughout the world seem to agree with me, with over 170 companies, patient groups, and research institutions stating that a moratorium is necessary. Nature and Science, two of the world's most influential journals, rejected the paper due to its ethical dubiousness.
Just as choosing whether or not to pursue such research will always remain a difficult choice, it is inevitable that this sort of research will continue to be attempted. It doesn't matter if 1000 research centers say that it is dangerous - it only takes on lab. The argument can certainly made that unless we try these techniques in actual humans, we'll never truly know if they work or not. There is only so much that you can do in a laboratory before one needs to make the scientific leap. This leap has been taken many times throughout the history of science, and it's always fraught with the unknown.
Take, for example, Edward Jenner. His name may not be familiar to you, but his invention of the vaccine has saved millions of people around the world. How did he discover this? He inoculated the 8 year old son of his gardener with pus from a person with cowpox, then challenged him with the virus. This worked beautifully, but it certainly seems a little ethically questionable, don't you think?

Figure 2: Edward Jenner advising a farmer to vaccinate his family
Of course, we know better now. We have better informed science, and we have better models upon which to test our ideas. So when will we see the successful correction of a mutation in a human embryo? Only time will tell, but I can guarantee that it'll happen sooner than you think!